Digital tools may give us an edge we need in the fight against the coronavirus pandemic.
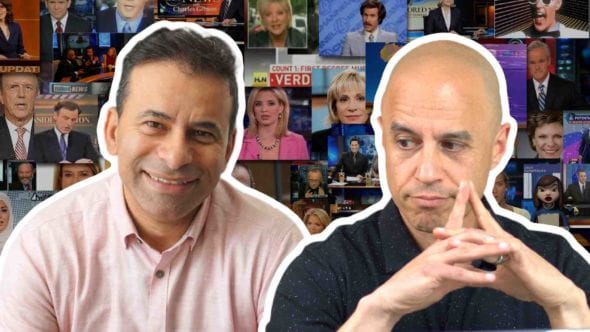
Dr. Eric Topol is a leading voice advocating for physicians and for integrating new technologies in our care models.
We talk about the current state of the pandemic, our failure to test early and its ramifications for our future approaches, the tension between privacy and effective public health tools, the new Detect study at Scripps that utilizes wearable devices to track the outbreak nationally, the paradigm shift that coronavirus is causing in our remote medical care models, the cardiac ramifications of COVID-19 disease, and much more.
Enroll in DETECT here.
Follow Dr. Topol on Twitter.
ALL our coronavirus coverage is here.
– Hey guys, it’s Dr. Z. Today, I have a very special guest. Dr. Eric Topol is a legend, he’s a cardiologist. He’s the editor-in-chief of Medscape. He’s the head of research at Scripps in San Diego. He is one of the great medical thought leaders around the intersection of technology and medicine. And now with our COVID-19 epidemic in full bloom, he’s joining us today to talk about things we can actually do from a technology side to make things better, Eric, welcome, man. It’s great to see you.
– Oh, it’s great to be with you, Zubin, thanks so much.
– So are you in your undisclosed bunker, remote location?
– Yeah, just not to leave home, that’s the key. That’s all we can do right now since so much of this had been botched up.
– It really has, just to quickly start, what do you think is the biggest thing we did that botched this thing up?
– Well, it’s unquestionably the delay in doing any tests for almost two months which is amazing. Because when you think back, we already had a patient diagnosed by January 21st in Washington, the same day as in South Korea, they did in the next couple of months before we got started, they did over 200,000 tests, they tracked every contact, hey did systematic testing, and we did basically zero. So we let the outbreak take over, and now, we’re seeing the consequences of it. So now it’s like, we’re so far behind the eight ball. And, of course, we’re seeing now a death toll and case because of the profound spreading and the question is, how can we cope with it? How can we try to address it?
– Absolutely, do you think if we had done what Singapore and Hong Kong and South Korea did early on, we might have had more targeted measures than we’re having now, where we’re having to institute more broad draconian measures late?
– Exactly, Zubin, so South Korea is probably the model but not far behind Singapore, Hong Kong, Taiwan, and even in China. Although they didn’t get the testing done as quickly as they would have liked to, but they did get into lockdown mode pretty fast, so relative to where we are. So yeah, Asia has led the charge, particularly South Korea, and they are a model for having flatten the curve and achieve this control of the outbreak. That is the containment phase, instead of the mitigation aspect.
– Yeah, the containment phase, and the question then becomes because you’re kind of an expert on this, one of the leading experts on this, they use an app, right, to contact, or to trace contacts and things like that, they use technology that some in the US would feel invades privacy, but there was quite successful. Can you talk about that at all?
– Yeah, you’re bringing up a really good point. This might not go over well in the US, and it’s obviously a little different in Asia, but for each of the South Korea contacts that have had any contact with a infected individual, they went through their records, that is, every transaction, every business, every sale, every, wherever they went to track every contact. Now, can you imagine? That’s probably not gonna happen too quickly in the United States.
– Is it not going to happen because we’re culturally opposed to that kind of thing or we just don’t have the technology or both?
– Well, I think, it’s both. I mean, actually, the big story today in the Economist, cover story’s about the invasion of privacy is a means to work towards control. I mean, there’s two big dilemmas that we have seen in this pandemic. The first was the economy versus the health of the public and the lockdown and basically shutting down the economy to preserve, prevent the spread and preserve lives. But the second one is the one we’re facing right now also, which is invasion of privacy. So we can try to trace spread, prevent spread versus what we have enjoyed largely is the lack thereof. That is, it’s the liberty and the extent of privacy in the US, which is much more than throughout Asia.
– Yeah, and I don’t think you can overstate this tension in the American psyche. We have a moral palate in this country that’s a little different than Asia. We do value the individual a little bit more in that sense. And so there’s the tension, but now what’s happening, Eric, is because we value that, we’re paying the price in our liberty to actually continue to go to work, to continue to go to school, to not be trapped in our houses, so it’s a trade-off. And the Italians are seeing that too, although we’re starting to see cases, that increase in cases level a little bit off in Italy, and so hopefully, their aggressive measures are starting to bear some fruit.
– Right, I mean, I think we’re seeing the first signs that Italy may have peaked, at least for now. And that’s, of course, encouraging, but the death toll they’ve had there as well as the overrun of all their hospitals in the Lombardy region in Northern Italy is just extraordinary. And we’re starting to see in New York a steeper curve of that than even in Lombardy or Madrid, the two hottest other areas in the world. So it isn’t looking good. The spread, as it turns out, was probably a lot earlier than was known here, because there was no testing, and it may even have antedated, of course, quite a bit than the January 21st date, because we just saw from Italy yesterday, that the first patient was probably January 1. That is, even though the first diagnosed patient was February 20th, almost two months later. So now we’ve had this virus basically incubating in countries outside of China for some time, and that means there’s a lot of spread.
– Well, and I think, what you’re getting at is a good pivot to what we’re gonna talk about today, which is without data, without the testing, without not being able to trace contacts, without being able to do aggressive local quarantine, without being able to institute measures that are more surgical, we are flying blind, and we’re way behind the curve. So what we’re seeing in New York is now this exponential rise because the thing was spreading there silently for weeks. And we’re gonna see probably when we do a post-mortem on all this exactly how bad it was. But now, you’re working on something, and the reason we’re even hopping on a call is that you emailed me the other day, and you’re like, “Hey, we’re doing this thing. “Any thoughts on how we can get the word out?” And I’m like, “Oh, yeah, I have thoughts. “We have a little platform, let’s have a conversation,” and you graciously took some of your time to talk about it. Tell me about what you’re working on, and then we can talk about more details on this.
– All right, well, right now, we know that there’s gonna be a lot more outbreaks going forward. And we’re just seeing the beginning arc of this horrendous pandemic in the US. So the question is, how can we get ahead of it? Because we can’t go out and get 330 million people tested now, not just for the virus but also for the antibodies to the virus. So what is a better way to do that at scale? And so what we thought was, recently, we published that we could use the Fitbit to predict the flu. We published that at Atlantic Digital Health just in February.
– Wow.
– And better than the CDC can predict or at least as good, and that was in 200,000 people that had Fitbits. And we said, “Well, wait a minute, “we could do this for COVID potentially.” And so what we did is very quickly, within a matter of weeks, the team at Scripps and also our tech partner at CareEvolution put together an app, put together a protocol, got it IRB approved, it’s called DETECT. And what that does is anyone who joins will be getting their smartwatch, whether it’s an Apple Watch or a Fitbit, the data will go to the servers to monitor whether their resting heart rate and other metrics are changing. And so we know that if there’s a cluster in the US where the resting heart rate is increasing, that would likely be the sign of an infection. Now, of course, it could be flu, it could be COVID, most likely, it would be COVID right now, but we think we’ll have an ability to find an outbreak before it spreads, and that is important. Now, the difference, Zubin, is there has already been validation of this tracking story, as you probably saw with body temperature.
– Yeah, yeah, with Kinsa, the device, right, that’s measuring, yeah.
– And they showed that you could get, for example, they predicted things were happening in Florida before they actually really got going. So that’s body temperature, but the problem with body temperature is you got to buy a Kinsa thermometer and you gotta take your temperature at least once or twice a day. Now, that’s great, but the problem is there are no thermometers of Kinsa or other smart thermometers even available right now. No less, the smartwatch is passive. I mean, you just wear, you don’t have to do anything. And we know there’s about 80 million Americans that have either an Apple Watch or a Fitbit, so if we got that data in a large proportion of Americans, it would be like your traffic map, the cars are sending a signal to see what the roads look like. And then we could get the same sort of read throughout the country about where is an outbreak likely to start moving. And so that DETECT app is, we just launched it yesterday, March 25th. And we already have had thousands of people join. We need to actually, the larger number, the better. More people we have, the better we can track the, it’s a research protocol, so there is a consent. There is voluntary sharing of data. But just to emphasize since we already started talking about privacy, Zubin, these data will only be used for this purpose, never otherwise be transferred or anything else. So this is a COVID-specific goal. We use the term tracking virus outbreak because we don’t know it’s gonna be COVID, of course, we just know that it’s likely to track a virus from our prior work, and we don’t wanna presume that we’re gonna make the diagnosis. But hopefully this will be a segue to that.
– Okay, oh, wow, there’s so much great stuff there. I’m gonna try to parse this down for my very primitive monkey mind and hopefully for the audience.
– For the first from the trip.
– And I wanna make sure that if I say something that is incorrect, that you interrupt me, okay? So let me see if I understand this. With a Fitbit or an Apple Watch, those are the two main devices you’re using, correct?
– Right.
– If people download the DETECT app, and we’ll put a link in for that and also put it in text on this video. With that app, they sign a consent, it’s part of a research study, so it’s IRB approved. So it’s gone through this, you do say, “Okay, I’m gonna give you this data, “but it’s gonna be used for this purpose,” right? And the point of this is that if you’re passive, there’s 80 million people with these devices, if you’re passively wearing the device and it’s measuring your heart rate and the reason we choose heart rate is that heart rate correlates somewhat to temperature and to illness.
– Before, it happens before amazingly.
– Okay, explain that to me. So even before you start getting sick, your heart rate is the first indicator like the canary–
– The heart rate antedates the fever.
– It antedates the fever, so it comes before the fever. See I took Latin, Eric, so your big words.
– As you know, the stress of a body, it first manifests through the heart rate, and then later, you’ll see the body temperature go up. And of course, it goes up even more with fever. But, yeah, no, it’s a really early sign. And it’s so easy to capture from a wrist.
– And that makes a lot of sense. Of course, since you’re a cardiologist, everything’s about the heart, Eric. I just want you to know that. So the early increase in heart rate then, if you catch that at a population level, this is why that’s so important in my mind because now the things we talked about were what’s our exit ramp from this draconian response that we have to have now because we dropped the ball early on with lack of data. Well, if once we start to tamp it down, we can watch the emergence of hotspots and target new measures locally and surgically that use technology, use local quarantine, contact tracing, and social distancing locally to get these little pockets under control because we know there’s a second wave that comes, we know that even if you control the first, you will get reinfection and re-outbreak if you don’t stay constantly vigilant. And it will help us understand geographically the spread of this outbreak much better than we can now because we have no data, we have limited testing, and terrible, terrible data. Did I summarize that correctly?
– You were spot on, Zubin, not surprising.
– No formal training. So the website is DETECTstudy.org, correct?
– I think that’s right, yeah.
– You think, that’s right. And so what I’ll do is I’ll send people there and this is the call, let me just give them a call to action directly. Guys, if you go to this website and download the app and follow the instructions and sign the consent, and you have a Fitbit or an Apple Watch, you will be doing your part to help during this outbreak, period. You will help our understanding, you will help save lives, and this is that important. So let me just interrupt right now and say please do this, okay? And we’ll put links in the description. Back to you, Eric. So you guys got this done in record time, were the bureaucratic? Was the bureaucratic activation energy lowered for this or did you just make it happen through sheer force?
– Well, it’s just amazing crew that are working on this that, this was a lack of sleep for a couple of weeks. And, you know, we’re very lucky at Scripps to have such a cooperative Institutional Review Board, one of the most agile in the country. So a lot of things came together, a lot of amazing people on the team. And of course, it was only because we had done that collaborative work with the Fitbit data set. Jennifer Radin was leading that project that we knew that there’s something really promising because the data there was so striking for predicting flu. And just going back on that, Kinsa was using that to predict flu outbreaks. And now they’re using this temperature saying, “Oh, well, there’s this outbreak in Florida, “but that’s not the right time for flu season, “so it must be COVID.” And so basically, we know this is gonna help but there’s other things that this could lead to. To emphasize, this pandemic is gonna go on for particular, this particular virus for at least 18 months, if not a couple of years and so for all that time, even when we do see some breaking the chain and flattening the curve, it’s gonna come back. And so we established a means of passive surveillance at scale. We can stay ahead of this because once you find a cluster and you maybe it’s wrong, if it is on the money, if these people, group of people are experiencing resting heart rate because of COVID, you can get in there and you could trace contacts, you could have precision isolation or quarantine. So there’s a lot, instead of this blitzkrieg approach, this dumbed down approaches, everybody got to stay home for the rest of the next few months, which is what we’re looking at right now, it’s a much approach. The other thing, Zubin, just to mention is, if we do get a drug in the months ahead, this could help direct their drug. If we do get other sensors, like for example, there’s a sensor now that you can put on the chest. It can detect cough, respiration rate, heart rate, and body temperature. We could send those out to people where it looks like there’s something going on. So there’s all sorts of things that this sets up once we can get to the group of people, the right zip code, where there looks like there is something going on.
– I’m a firm believer in this and in fact, there are devices in place now in our home that listen to us. And whether it’s a Google Nest or whether it’s a Vivint Alarm System, or whatever it is, those systems can actually be equipped with algorithms theoretically that can recognize sounds of respiratory distress, changes in vocal patterns, other things like that, that can actually alert people that are in home quarantine, even if you’re wearing a wearable oxygen monitor, other things like that, can alert your clinicians that, hey, there may be a decompensation, because one of the interesting things that we see with this particular viral pattern is that people are doing okay for about a week, and then suddenly, they’re short of breath, they even have silent hypoxemia. And then they show up and you’re already behind, they’re intubated, the next thing you know, it’s ARDS and they’re in a prone position fighting for their life. So there’s so much potential for technology, but the tension between people listening to us in our homes and safety is an eternal one. I mean, how do you personally think about that, Eric? Because I know everybody has their opinion on it, but what do you think about that tension?
– Well, I think, this is a time that we’ve never seen before. It’s our show really, especially for those who have family members who are in the hospital, and maybe they’re in the ICU, and you can’t even see them. I mean, this is just, it really is a nightmare. So that’s when you start to think, “Well, what can we do to try to?” We got so far behind as we discussed in the beginning. But what can we do now? It does surrender some privacy. It seems like the appropriate trade-off. It’s just like in medicine right now. I mean, who wants to go to your doctor? This is not about COVID, this is about just an appointment. Who wants to go to our clinic and sit in a waiting room or go in a hospital that, you know? So we’re at a turning point in medicine and it’s the same thing for, how do we counter this big crisis that we’re confronting?
– It’s interesting because I think, this will, this COVID pandemic is going to have profound, long-lasting cultural shift changes across society, but medicine will be the most specific. And I think, you and I agree on a lot of things, Eric, and when you wrote that New York Times op-ed on physicians having to band together to fight what is destroying medicine, the corporatization and the commodification of our profession. And yet, you will also embrace that technology is a crucial part of how we move forward. Well, now we’re getting there, because with COVID, what we’re gonna see is there’s gonna be more telehealth, there’s gonna be more digital devices, and instead of us fearing them and wondering how we’re gonna integrate them into our practice, we’re gonna use them, leverage them to enhance the human analog relationship that underlies all of it. And so this is the chance, right? If we don’t capitalize on this after this is over then I think we’ve missed a huge opportunity and also to get paid to do those things, because those business models have not caught up with the reality on the ground. I have an iPhone that can do more than Epic can do, right?
– Yes.
– Easily and yet, because of HIPAA regulation, the fact that we don’t get paid, all these other things, we can’t make it work. I mean, what what are your thoughts on that? Because this is really right in the wheelhouse of what you write about in your books, and and all of that.
– Well, you have a lot to unpack with what you just said. There’s just so much there. I mean, firstly, from the physician and our healthcare workforce standpoint, we have been basically managed by administrators. We’re the only profession that doesn’t have its own people that are directing things. And we’re in this disaster of no protective equipment and just sitting ducks, sitting ducks.
– Oh, by the way, Eric?
– Yeah?
– So Eric, we’re sitting ducks, but who’s to blame for that do you think? Like–
– At the governmental level, once you see the WHO alert on January 3rd, that there’s going to be a pandemic, you might wanna stock up on equipment, you might want to check that, “Oh, you have a test ready?” You might wanna say, “Oh, do we do we have any masks in this country? “Do we have any shields? “Do we have anything?” So you might, of course, there was no pandemic group, because they were disbanded a couple years prior. So, yeah, but then at the hospital level, the hospitals, they can they can have their own reflexes to see, “Hmm, there’s something very serious going on in Wuhan.” And you know what, people fly every day from Wuhan to the United States. Maybe we ought to get our health system geared up here. None of that really happened. It wasn’t taking this seriously in retrospect. But the other problem that you’re getting to is telemedicine 2.0. Because today, of course, you mentioned that the reimbursement’s an issue, there’s regulatory issues, this this cockamamie thing about, “Oh, you have to have a license in this state “where you’re seeing the patient.” I mean, that’s the whole point and there should be a national licensure, of course, and here it is, but it isn’t respected that is taking the exam. But the point there is, right now, it’s a video chat. And it doesn’t need to be a video chat, we have to recognize that this distance doctrine is going to be more than norm. And you can equip the sensors, like, for example, you could diagnose a type of pneumonia through the microphone of your smartphone with an AI algorithm. There’s all sorts of things that you can do. I mean, you can image your entire body except your brain with an ultrasound probe connected to a smartphone, my goodness. So we’re not using this type of technology nearly as we could. And that will take us to a different type of telemedicine because we could still be at a distance, but most of them relevant physical exam could be obtained. In fact, continuous data beyond just a one off physical exam. So that’s where we can look to in the future.
– Yeah, I’m a believer in that as long as we retain some of that human touch and human connection at the heart of it, I agree. Well, one one thing, Boris, I think, it was Kasparov said about AI, right? It’s a famous line of his. He said, “Yeah, yeah, the AI can beat me “and pretty much any human at chess. “But if you give me that AI as a tool, “I can beat everything extent. “I can beat computers and humans.” And I think with medicine, with doctors, it’s the same thing. Give us the tools and we can do wonders that no computer AI will ever replace. So I think that’s where the future is, and I think this pandemic, if there’s any silver lining, it’s gonna be that that we’ll actually see that happening.
– And I couldn’t agree with you more. Garry Kasparov’s a hero of mine and his book, “Deep thinking”, gets right into your point. The idea though, is the human touch is essential, it’s the essence of medicine. We have to sacrifice that a bit when we have this problem of asymptomatic carriers, at least 30% of our population is an asymptomatic carrier. And, of course, many of those will have the antibodies that hopefully will neutralize, we don’t even know about that. The ability for spread, the ability for reinfection, we don’t even know how long they last. But while we’re in that zone of uncertainty, we have to start to, imagine getting sick right now with a non-COVID illness.
– Yeah, yeah.
– And the fact is, we have a real problem in delivering care, because our our healthcare workforce, if it isn’t just stressed out so profoundly in certain places like New York, now Detroit and Louisiana, New Orleans, and many other locales, it’s gonna be many other places in the weeks and months ahead. So that’s why we should build our distance capabilities as much as possible now.
– Absolutely, and one thing that very few people are talking about is our colleagues in the outpatient world who do elective surgeries for a living, or see patients that are well are relatively well, and this is their bread and butter are potentially going to go out of business. They have to pay their staff, and if they don’t have a means to see these patients remotely and get paid for it, they’re gonna become part of the economic casualties of all this, which, it would be tragic, because as it is, we don’t have enough manpower in healthcare. So it’s a huge problem.
– You’re absolutely right. And we’re talking about at least a couple few months in this state, and as you say, people, the surgeons and proceduralists that rely on elective procedures for their work, they’re really gonna be in pretty tough shape for now. Eventually, we’ll get back but then, then the problem is how many more months before this cycles back in?
– Right.
– So this is, a lot of people don’t realize we’re looking at a long story here. We like to be optimistic. You and I are both optimists. But unfortunately, the reality is one that’s much tougher than what we like.
– Yeah, so we have to bring all our tools to bear on it. And we also have to speak, I think, you and I, particularly as public figures have a responsibility to speak rationally and commonly about this stuff, and say, “Okay, here’s some actual ideas “for what can happen, “and that’s what I see you doing right now,” which is wonderful. And by the way, I wanna thank you too because your genomics conference that you host in San Diego, you invited me in my early days, and it was really formative meeting the amazing people you have there talking about the intersection of biomedical science, science, genomics, personalized medicine all together, and it really opened my eyes to that and you’ve been really early supporter of the work we’re doing and so such a seminal figure in healthcare, Eric, I want to thank you, like, I’ve not gotten a chance to thank you personally for that.
– You’re very kind, you’ve inspired us. I think, we’ve had you a few times to that conference in the 12 years we’ve had it and I don’t know of anybody that can present and captivate an audience of physicians and scientists like you, Zubin.
– Man, well, your five bucks is in the mail for that nice compliment, thank you. At this point, we can take any revenue we can get. So I think if we’re gonna wrap this thing up, I’d love to hear if you have any thoughts on the cardiac sequelae if that’s something you can speak to of what we’re seeing in patients with COVID-19 in the ICU. There’s been a lot of reports that at Washington State, that it’s cardiac failure, whether it’s cardiomyopathy, whether it’s asystole or V-tach that is killing a lot of these patients often suddenly even in the throes of their improvement and excavation. Any thoughts on that?
– Yeah, very important point. I’m glad you mentioned it. We basically have thought this is a long story than just the once the COVID gets into lower respiratory tract, it wreaks havoc. But it actually does have effects on the heart. It’s not entirely understood, but a report just came out yesterday in JAMA Cardiology. 17% of the patients in the ICU setting had a myocardial damage. And as you said, there’s several reports of cardiomyopathy. So the question is, is this related to hypoxia? Is it related to the primary lung problem? Or is there a direct hit of the virus to the heart? A lot of that stuff is a little fuzzy, but you’re right about arrhythmias, And the idea that you would take drugs like chloroquine that can make a QT interval worse, which has no data to support it, these are crazy things. So we have to respect that there is a cardiac story that’s unfolding, it’s not completely sorted out. We also do know that there’s been a lot of flap about ACE inhibitors and angiotensin receptor blockers, which are obviously, as you well know, commonly used in hypertension and management of heart failure. And those drugs, there’s still no resolution. Could they help, could they hurt? This paper is going both ways, but it’s all a bunch of unknown. It’s in suspension. So no one should have those drugs discontinued. But I think the most important point is there’s a direct evidence of heart damage in not an insignificant number of people. That’s very troublesome and we have to learn more about that.
– Yeah, thank you for that insight. I mean, and the idea of the quinine drugs being pushed, they can cause heart arrhythmias and QT prolongation and things like that. It’s very concerning in the absence of really good data. And there’s stories and reports around the country of doctors trying to prescribe this stuff and hoarding it and I think those are just bad eggs. It’s not like the majority of us are that dumb.
– No, no, you’re right.
– Yeah, exactly. And your thinking on ibuprofen and the flap around ibuprofen.
– It’s kind of like the ACE inhibitors. It’s much ado about nothing, it’s just nothing there. It was a fringe group that put out a concern, but when you look at all the data, that story on ibuprofen and other NSAIDs, it just doesn’t have anything to back the stopping those drugs. I mean, there’s just, it’s so flimsy. All this stuff, whether you see it on Twitter or from Trump or wherever the source, you have to be really suspect ’cause there’s just no real evidence.
– Yeah, yeah, I’m with you on that. That’s what I’ve been telling people as well. And the more I look into it, the more I’m convinced that’s true. So in terms of the call to action here, Eric, I think, I’m gonna double emphasize that people go to the website that we’re gonna link right here again in the description, et cetera. And if you have a Fitbit, if you have an Apple Watch, you can download this app and be a part of a solution here. And I wouldn’t pitch a BS app to you guys that I thought was just gonna steal your data and give it away. This is Eric Topol we’re talking about it Scripps with a great group of researchers. And if there’s anybody you should trust with that data, it’d be these guys and I’m telling you that as someone who’s known Eric for a long time, and he is one of the true heroes of medicine. So, Eric, any parting thoughts or concerns or wisdom for what we should do in these uncertain days ahead?
– No, I think we’ve gone through it. I really appreciate your support on this, Zubin. You’re amazing and we won’t let the folks down that are part of this DETECT project. Hopefully, if we get a big proportion of Americans on it and spread the word, they’re not just joined, but hopefully, let everybody else know we can get on top of this to an extent, and change its natural history ’cause right now, that doesn’t look pretty at all.
– Yeah, but you know, Eric, I’m with you though, I’m an optimist and I think, if we make enough noise and we make sure we keep putting the pressure on science, the crap out of it, we’ll actually get there. It’s just we’re a little behind. So now we gotta apply the brakes even harder, and do a little more math, but we’ll get there and your–
– I love that science the crap out of it, I’m with you.
– So we have a, as a side note, Eric, we have a supporter tribe on Facebook and YouTube and so they subscribe with like a small monthly fee to get uncensored access to me doing live shows. And there’s a group, there’s a couple of nurses in that group that created a whole set of T-shirts for the supporter tribe and one of them just says, “Science the crap out of it,” and it’s gotten. So it’s a movement, it’s a movement. That all being said, Eric, it is a, as you know, look at me, I’m unconsciously rubbing my face, which is the one thing you’re not supposed to do. Luckily, I sterilize myself every five minutes in this house and don’t leave it. Let’s keep up the social distancing. People need to really listen to that. Thank you again for being on the show. You’re, again, a personal hero of mine and to many out there. And guys, ZPac, please do me a favor, go to the website that we’ve listed. Share this show, become a supporter on Facebook or YouTube, subscribe, especially on YouTube, click that little bell so you get notifications ’cause we’re not, we can’t stop, won’t stop when it comes to this coverage. And thank you Dr. Topol and everything you guys are doing down at Scripps. Stay safe out there and we out, peace.
Category
- The ZDoggMD Show (829)
- Featured Videos (189)
- Doc Vader (142)
- Against Medical Advice (128)
- Medical Humor (95)
- Public Service Announcements (87)
- Music Parodies (74)
- Nurses (59)
- Meditation (57)
- The VPZD Show (38)
- ZVlogg (36)
- ZTalks (28)
- ZBlogg (24)